

Atop the Covid Plateau
Atop the Covid Plateau
our hyperendemic future

WARNING: the narration gets a little… angry. Preventable deaths, gaslighting, and lies piss me off.
When I last wrote about covid in Canada, just a couple of weeks ago I expressed a good deal of uncertainty about the future: would it be an endless series of distinct waves, or a high-level plateau?
After doing some more analysis, I’m leaning fairly strongly toward the latter. This is a state that is sometimes referred to as hyperendemic: “persistent, high levels of disease occurrence”.
This is how Bayesians think. Non-Bayesians are desperate for closure, for the illusion of certainty. Bayesians aren’t bothered by uncertainty any more than we’re bothered by large bodies of water: these things exist, and are necessary for life. Pre-scientific philosophers are like hydrophobes: when confronted by the ocean of uncertainty they went off in search of the high desert, and then wondered why everyone was dying of thirst. Bayesians learned how to sail, and then how to swim.
What bothers a Bayesian is a set of answers to a question that all look about equally plausible. It makes it difficult to plan our day. To stretch the analogy, these are the equivalent of fog at sea. We don’t know which direction to move in.
So I keep coming back to questions that are wide open, trying to get a little more insight into what is most plausible. What will happen with covid in 2023 is a question of general interest, if this lie-filled exercise in gaslighting from the CBC is to be believed:
Omicron rapidly shifted the need for boosters across Canada in a desperate attempt to protect the vulnerable and fend off worsening spread of the variant, but by early January COVID hospitalizations had reached record highs in much of the country.
Despite our best efforts, Omicron was a runaway train heading straight for us.
"I'm not really sure what could have been done," Fauci said, when asked how countries around the world could have better prepared for the impact of Omicron, given that even China has failed to contain it with draconian public health measures.
That’s a lot of lies and gaslighting. There was nothing desperate in our attempts to ward off omicron, which was met with a grab-bag of incoherent and ineffective measures, at least in my home province of British Columbia. There was a nominal mask mandate but N95s were not mandated and masks did not have to be worn while sitting. Dancing was prohibited, so the Puritans were happy, I guess?
No one who understands the aerosol nature of respiratory diseases would have enacted such a program, which is not a “best effort” but rather managed to be both ineffective and needlessly obtrusive. So if by “desperate” we mean “stupid”, I suppose we can call this desperate. But I don’t think that’s what “desperate” means.
Finally, if Fauci isn’t sure what could have been done, when literally every engineer who has studied the problem knows that universal indoor public N95 mandates with a crash program to improve or install indoor public ventilation, filtration, and UV systems would have saved thousands of lives, then he’s just incompetent. Never put a physician in charge of an engineering problem, and respiratory health is an engineering problem.
There’s also something called "population immunity" that is mentioned in this terrible article. There is no such thing for covid. Immunity to omicron wanes on a scale of a few weeks to a few months. Nothing else can explain Canada's four covid waves in 2022, which peak at about 95 days apart. This article is pure propaganda by the organs of the state. No wonder nobody trusts experts any more.
The focus on vaccination alone as the answer to covid is a lie spread by physicians who are ignorant of basic science and engineering, and for that matter ignorant of basic data on covid: vaccinated people can carry and spread the disease only slightly less effectively than non-vaccinated people. So why were we checking vaccine passports in late 2021 and early 2022? I mean, I did at events I ran in the early days, before the data was in. But once it was, I stopped, because I knew it was obtrusive and largely useless. N95s on the other hand are effective: you can’t catch a virus that doesn’t make it into your nose or lungs.
So where are we, when we strip away the gaslighting and lies by authorities?
We are here:
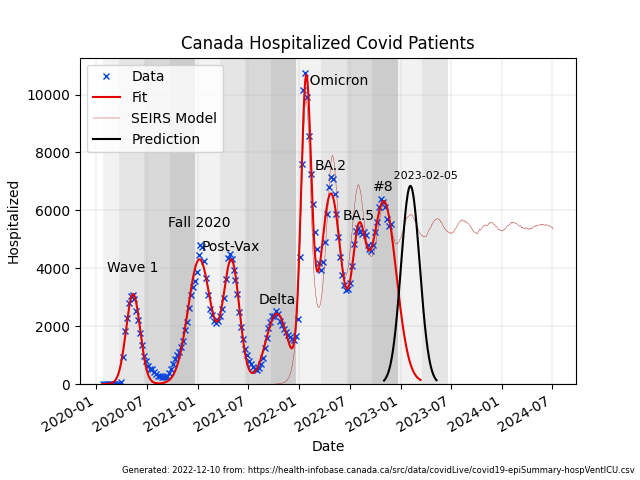
This is much like my previous analyses but for the addition of a little more data and a new curve, which is the outcome of a numerical model of pandemic spread that I wrote to better understand the dynamics.
It is a very simple example of what’s called a SEIRS model: susceptible/exposed/infectious/recovered/susceptible. Those are the states an individual in the model can be in. The model population is a hundred thousand individuals on a 250x400 grid.
When more than one individual is on the same grid square and one of them is infectious, any susceptible individuals sharing the space have a fixed probability (17% in the model, for various reasons) of becoming infected, which moves them to the “exposed” state. The exposed state lasts between 1 and 7 days--this is based on the data, with says people become infectious after about 3 days on average, with a few days variation--and then the individual becomes infectious, which lasts between 3 and 30 days, again based on the data. These are crude numbers, but I wasn’t looking for exactitude. It just kind of happened. Once an individual has recovered they fall back in to the the susceptible state in 15 to 60 days, which is the only way to get waves that are spaced the way the omicron waves are.
The model progresses a day at a time: every day all individuals move a random distance based on sampling a 1/r-squared distribution with a scale length of 3, so the infection tends to grow in neighbourhoods. The simulation is seeded with about ten infected individuals on day zero and runs for 1000 days.
There aren’t very many free parameters: the infection probability and population density are reciprocal with each other, so they are both poorly defined. Within broad limits, higher density is the same as higher infection probability. I selected them based on producing waves that looked roughly like the ones we have. If the infection probability is too high or two low you get waves with troughs that aren’t like those observed. As it happened, to get ones like what we see in 2022, you end up with diminishing amplitude, which produces a hyperendemic state.
The waning times are fixed by the wave period, and to get waves with an average of 95 days between them immunity has to wane in the range of 15 to 60 days. The lower end is more important than the upper. There is some arbitrariness to this, but there is no model in which waning does not occur on a scale of weeks to months that can reproduced the observed wave frequency.
And as a reminder: both the 7th and 8th waves in Canada were almost pure BA.5, so they were not driven by new variants. The evidence strongly suggests it is waning immunity alone that is driving these waves.
Let’s take a closer look at the raw hospitalization data with nothing but the model fit. The model has been scaled and shifted to match the omicron peaks, but is otherwise as generated. And again: there isn’t a lot of freedom in the model parameters. The general shape of the troughs constrains the infection probability for the population density, the period constrains the waning immunity parameters, and everything else--time to infectiousness and recovery and so on--is constrained by the data. I’ll probably go back this week and re-run the model in a more systematic way now that writing it up like this has clarified my understanding, but I’m fairly confident it is as realistic as such a simple-minded system can be. And this is what it looks like:
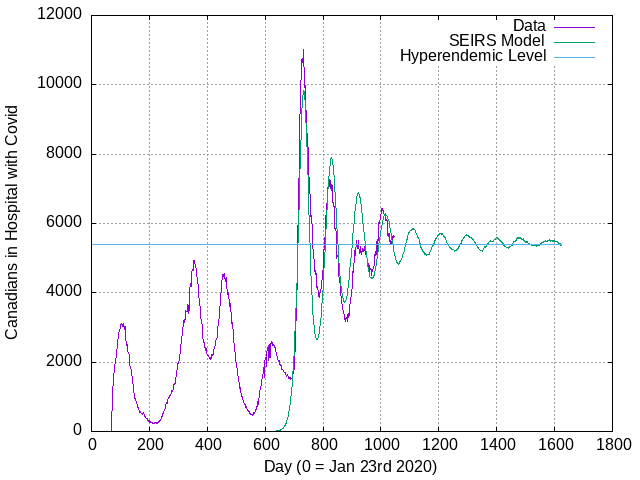
That doesn’t mean it’s correct, mind. You can already see the suggestion of the next wave starting to rise, a little earlier and a little higher than the model would suggest. And obviously the fit is far from perfect. “Prediction is hard, especially with regard to the future.”
That said, I now think it most likely that Canada is transitioning from repeated omicron waves to a hyperendemic level where there will be around five or six thousand Canadians in hospital from covid all the time, for an average of 15 days apiece, resulting in around 134,000 individuals hospitalized every year (at a cost of about a $350 million, if that matters).
About 18% of people hospitalized for covid die, causing 24,000 direct deaths from acute covid and a high rate of indirect deaths from heart attack, stroke, etc, in the months following infection. Oh, and disablement and immune compromise, too, resulting in high levels of deadly infections from other diseases, like flu, RSV, and strep A. Even without these additional effects, hyperendemic covid will persist as Canada's number three killer, behind only cancer and heart disease (it's about 1/3 the cancer rate, half the heart disease rate.) About 7% of Canada's hospital beds will be filled by covid patients at any time.
And that’s if evolution doesn’t throw us another curve ball. It is unlikely that any variant will show up that’s more infectious than omicron, which appears to be comparable to the measles. Measles is the most infectious disease we know of, and it’s likely that the basic physics of aerosol dispersal starts to limit the possibility of becoming moreso. There is also relatively little selective pressure to become more infectious than omicron because diminishing returns set in: once a virus has the capacity to infect practically everyone within reach of aerosol diffusion, there’s not a lot to be gained by doing better. Viruses have limited genetic resources, and those are better put to other uses, like becoming more immune-evasive. If a covid variant could trick our immune system into ignoring it completely it would do very well in the current N95-less environment, even if it killed the host after a few infectious days with 100% certainty.
There is very little selective advantage to becoming less lethal, so we can’t expect that. We can only hope that selection for immune escape doesn’t also happen to make the virus more lethal.
Hope is not a plan, unfortunately.
For people planning holiday travel and get-togethers: everyone should rapid test beforehand, no one should be invited who does not N95 in all indoor public places--because really, why would you invite someone to a Christmas gathering who doesn’t care about your health?--and CO2 should be monitored, with open windows to keep it below 800 PPM, and HEPA filters running regardless to keep the air clean.
We can beat covid with engineering mitigations. But first we have to admit that it’s still a problem, and be willing to do some really basic stuff like wearing N95s indoors in public everywhere while we implement those fixes.
If we care about each other, we will.
If we don’t, we won’t.
Another excellent article, Tom! Although I fear you’re just a still small voice crying out in the wilderness...to our societal detriment. I’m still masking everywhere. 👍
Thanks for another timely analysis of the current state of Covid-19 and your practical solutions as to how mitigate the risk of a respiratory disease during this Christmas season.