


The Effects of Reinfection
50% increase in hospitalization for the first infection, 500% for the next

With more people on their second, third, or moreth infection, it's worth looking at the effect of getting covid more than once. My intent had been to write about covid less this year, as I had given up on influencing anyone to do anything, but I'm starting to see a renewal of interest as people are figuring out that pretending the pandemic is over hasn't been an effective public health strategy. I'm also seeing news of more super-spreader events, from local concerts to major meetings of infectious disease physicians.
First, a note about priors, which are the beliefs we come to evidence with. The goal of Bayesian knowing is to update our priors in the face of new evidence. To do that, we have to honest and fearless, and not get attached to our priors, which are knowledge and therefore uncertain. The whole point of knowing is to change what we believe in either the "more" or "less" plausible direction. Sometimes it'll be one, sometimes the other. If we aren't open to both--which means "not being 100% certain-for-sure" either way--then we aren't interested in knowledge.
Holding beliefs without uncertainty is faith, not knowledge.
A significant and well-funded group of people have faith that "lockdowns" and N95s are to blame for everything bad that's happening all around us right now.
It is the nature of faith that those people will not be moved by anything I have to say here. Faith can't be achieved by looking at evidence and updating priors, so it can't be cured by that process either: it is a psychological state, not a logical one.
Despite this, many people are pretending to use arguments and evidence in favour of their faith that "masks" and "lockdowns" are more likely to have caused the ongoing flood of excess deaths and disablements than a virus that attacks the blood vessels and damages the immune system. Unsurprisingly, these "arguments" aren't really tenable.
For example, in my home province of British Columbia we had three months of reduced activity three years ago. In some places that's called "summer". Our mask mandates--like far too many of our masks--were loose. Claims that an entire generation of children were damaged by not wearing masks, as there were weak-to-no mandates for kids, for a short time while doing remote school for six weeks are extremely implausible, which means it would take a good deal of evidence to update my prior belief to the point where I think a few months of reduced social contact can explain anything. That evidence has not been forthcoming.
With regard to N95s, anyone who has ever worked an industrial job knows that wearing a respirator all day is routine, and newly-minted claims that masks are damaging in a variety of previously-unimagined ways have to be weighted against the evidence of generations of industrial workers whose lives and health have been saved, not harmed, by them.
Despite this, there are still people who are asking, "Do you think that getting a deadly, disabling disease more than once might be, well, kind of not good?"
The question smells like bias. You can tell by trying it on some other subjects: Do you think getting the flu more than once is bad for you? How about RSV, which kills a few thousand older people in the US every year, even though they've all almost certainly had it multiple times already? Or getting into car crashes? Any physiological insult, really: does the damage accumulate? Inquiring minds want to know.
No one asks those questions because no one is motivated to ask those questions by a desperate desire to not have to do anything at all in the face of a novel virus that is now and is likely to remain comfortably among the leading causes of death until we start cleaning the indoor air we breathe, which is a solved engineering problem we should probably put engineers in charge of in every workplace, including hospitals, because why wouldn't we?
But since there are a lot of people who want covid to be nothing much so they can go on pretending to care about people while actually doing nothing to help anyone, pondering if getting covid multiple times might be bad for you has become a bit of an industry, because wouldn’t it be lovely if it didn’t?
There have been two general outcomes of studies on covid reinfection: those that say it gets "milder" with multiple reinfections and those that say it gets worse.
As is typical for medical studies, the disparity in results are due to an extremely large diversity of study designs and little or no attempt to focus on any underlying objective reality. The studies measure what the studies measure, which can’t be compared to anything else.
As a physicist working in biology I've learned that biologists have a very different view of data than physicists do. When a physicist measures something we are almost always intending it to produce a reproducible estimate of what is happening "out there" in the world, which exists independently of our own minds, intentions, emotions, or measureing instruments.
Even in applied physics, where our measurements can be very apparatus-specific, there is a general acknowledgment that we could tie our results to an objective standard if we wanted to.
This is in fact sometimes done with field-specific standards. In the early days of real-time mega-voltage imaging--where the therapeutic x-rays that treat cancer are also used to form a video image of the patient's anatomy to ensure we're hitting the right bits--different groups wanted to compared how well they were doing, and so a standard phantom (anything imaged that isn't a patient is a "phantom" for some reason) was developed that anyone could have machined to spec, which would allow for images to be compared. At first there were just a couple of these made, which were shipped around between groups.
Many of the tools for meaningful quantification in biology are less than a generation old, and in epidemiology, as near as I can tell, hardly anyone has tried to conceptualize phenomena in a way that is even slightly independent of the specific tools of measurement employed. One day I may write up my "adventures with R0"--the "basic reproduction number" we've heard so much about--which is a text book case of a purely instrumental concept masquerading as something objective.
This lack of any attempt at objective standardization has resulted in different ways of investigating reinfections that produce very different results because they are measuring different aspects of objective reality with no attempt to clarify, much less standardize, what the differences are.
Two types of study that measure completely different aspects of objective reality are self-report surveys and hospitalization data. The former measure how people feel, the latter how they are.
How people feel is not unimportant, but is not a great measure of health or quality of life. I've talked a lot in the past about folk ontologies, and simple, straightforward reification of people's feelings is the ancestor of all of them. This is the folk ontology that asserts that if a person feels "that X" then "X" is the objective state of the external world, which is the kind of thing that gives us ghosts and demons. Feelings are facts, and important sources of information about the person having them, and nothing else.
For example, asking people about their experience of pain after getting knee-replacement surgery tells you how they feel about their surgeon, not about the pain-free range of motion their new joint has.
Self-report studies like this one done by the UK government tell you about the biases and preferences of your study population, not how objectively healthy anyone is. And it's not as if the notion of "objectively healthy" is some mysterious concept that no one could possibly define: there are plenty of people who are suffering with long-term or short-term conditions that prevent them from enjoying the routines of daily life the rest of us take for granted. An ME/CFS sufferer who can barely get out of bed is not objectively healthy. A person who can't roll over in bed because their back is screwed up is not objectively healthy. A person who can't walk without pain is not objectively healthy. And the existence of corner cases does not change any of that, any more than existence of beaches means oceans and land do not exist.
Bias about long covid is all around us. At this point in the ongoing pandemic most of us know someone who "doesn't have long covid" but does "seem to be sick all the time" or "has such low energy" or "really has trouble focusing". Those people all have long covid, and self-report studies that say there's a low incidence of post-viral syndrome in people who have had covid are measuring the effectiveness of social pressures to deny the impact that covid is having on every aspect of modern life.
Furthermore, we should pay more attention to studies that say a phenomenon exists than those that say it does not.
This is the way engineers think about things: 99.9% of planes don't crash but when one does we don't say, "But 100% of passengers surveyed in this self-reported sample survived their flight!" as if that absolved us of the need to do anything. We focus on the objectively real cases where planes did in fact crash. Which is to say, even if reinfections are no big deal in some populations, and their negative effects are not seen in self-report studies covering whole populations, they are still a big deal in the populations where they are a big deal. It's almost a tautology.
And if you care about people as opposed to people who aren't badly affected by covid, you'll care about this.
A very nice study of the latter type is this analysis of the US veterans database that was published last fall.
It's a look at (mostly) older white men (half a million infections, 40K with two or more, five million uninfected controls, 90% men, 70% white, average age 60 with a standard deviation of 15 years) and it does not bode well, at least if you happen to be planning to get old.
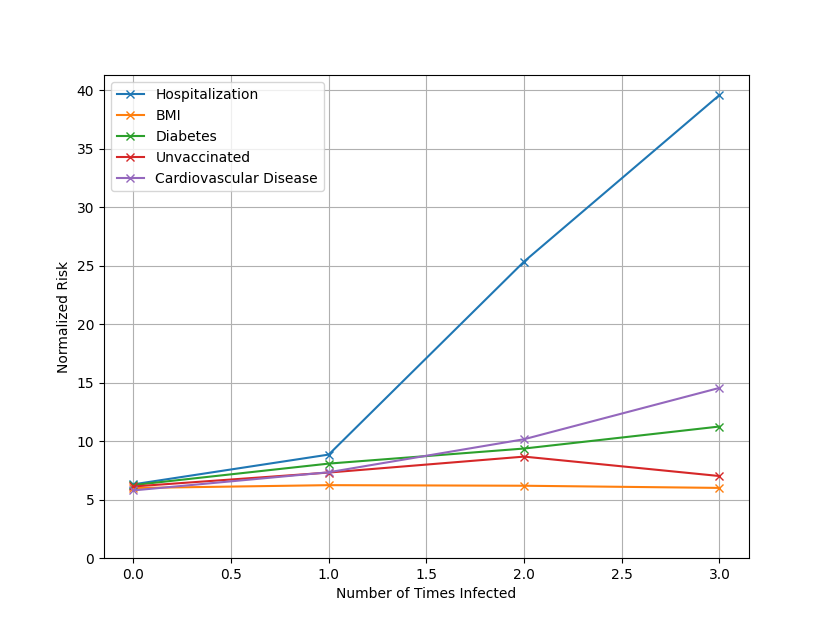
This graph, which I've generated from the data in the study, shows the percentage of people in each group (0, 1, 2, and 3+ infections) who have various conditions in the following year.

That is, the odds of being hospitalized for any reason in this cohort is about 6% (62 per thousand) in a given year if they've never had covid. The people in the study are older, and older people end up in hospital a good deal, even without covid. If they've had covid once there is a 50% increase, to about 9%.
Now, there are plenty of people who have no problem subjecting strangers to that risk so they can blend in with the herd while going around asymptomatically unmasked spreading a deadly, disabling, disease... but the risk jumps for the second infection to 25%, which is huge. It's an almost five-fold increase over baseline. For every 1000 people in the cohort who get covid twice, 250 of them will end up hospitalized for some reason in the following year, whereas fewer than 100 would if they only had covid once, or not at all. And after that the number goes up sharply. It's 400 out of every 1000 people who get infected three or more times. Forty percent.
Specific conditions like cardiovascular disease and pulmonary diagnoses also rise sharply after the first infection.
This is not like the flu, or a cold. It just isn't. No matter that you had it once and were fine, or your friend had it twice and was fine. Data tell us how the world is. Anecdotes tell us about the psychological needs of the person relating them, and nothing else.
While the infected and multiply-infected cohort are somewhat sicker than the uninfected controls, they aren't anything like sick enough to account for the observed differences: the uninfected cohort are healthier by a host of measures, although almost dead on in things like BMI (30 vs 31).
18% of one group having cardiovascular disease instead of 15%, or 3% with cancer instead of 2%, cannot account for 5 or 8 times more hospitalizations. It's mathematically impossible. Here I've normalized the percentages of a few conditions to the hospitalization risk for uninfected people to show the relative rise, and it's nothing like enough to account for the observed increase in hospitalization.
The things that do significantly increase risk of being in the multiply infected group are being immunocompromised and having been hospitalized during the first acute infection. Both of these are selection effects: immune compromised people are more likely to get covid multiple times now that we've abandoned the most basic protections for them, and they are also more likely to end up in hospital.
And acute covid causes immune dysfunction.
So my advice, especially for people like me who've already had it once is: don't be a libertarian sheep.
Dare to be different.
Don't let the freedumb crowd or the toxic positivists shame you into conformist behaviour that puts yourself and others at risk.
Wear an N95 when you're indoors in public, and most of all demand governments listen to engineers and scientists who are pushing for improved indoor air quality. Poke businesses and venue operators about what they're doing to protect people: HEPA filters, improved ventilation, and upper-room UV are not rocket science. They're known tech, not enormously expensive, and the way we get ourselves out of spending way too much time in hospital, and dying years earlier than necessary.
We don't have to accept this situation.
A hundred and fifty years ago people were shitting in holes in the ground and drinking water from adjacent wells and dying of it way too often. They didn't know any better, and once they did it took generations to modify every single habitable building to accommodate the wonders of indoor plumbing while building a huge public infrastructure to deal with waste processing and water filtration and chlorination.
For cleaner, safer, air we don't have to build anything like the kind of public infrastructure that was needed to clean drinking water and treat sewage. We just have to modify public buildings to improve on something that they're already doing. We don't have to wait generations and hundreds of thousands of avoidable deaths, and a much greater number of disablements, to get the job done.
All we have to do is understand that the problem is nothing but "provide about 10 air changes per hour of HEPA filtered air to every indoor public space," and commit the required resources to do it, which would save a huge amount of money as well as lives, all while reducing the misery of all airborne diseases, not just covid. One way of ensuring indoor air quality is to prominently display CO2 levels, which is also not hard.
Only a libertarian sheep--someone whose idea of "freedom" is "relentless conformity to the way we've always done things"--would be opposed to that. I believe such people are also known as “conservatives”, and if you’re not routinely wearing an N95 indoors public spaces that don’t have a CO2 monitor on display, you are a conservative.
Don't be a conservative. Wear your N95. Dare to be different. And push governments and businesses toward healthy, clean, filtered, indoor air.
Scary but thanks again for spelling things out so clearly …both the risks of multiple cases of COVID and the reasons people are resistant to that knowledge and acting on it.
I’m glad - and thanks - you’re saying it, but I fear nobody is listening...